ACL INJURY AND REHABILITATION
Add Your Heading Text Here
ANATOMY AND EPIDEMIOLOGY OF ACL INJURY
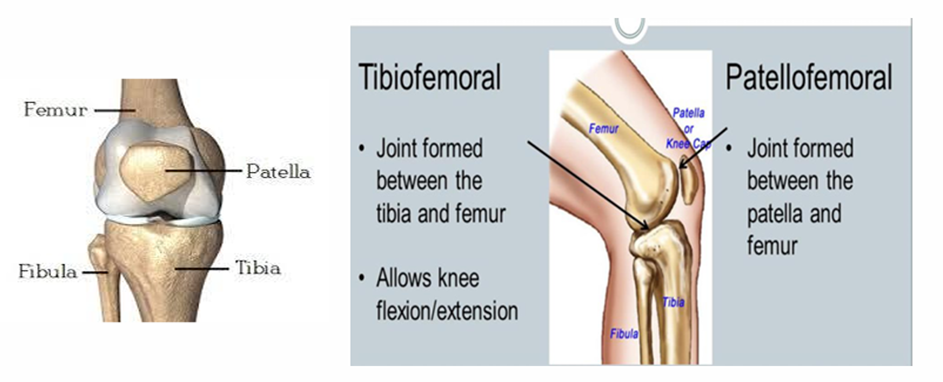
The tibia-femoral bone articulation forms the most complicated synovial joint, the knee. The medial and lateral condyles of the tibia and femur bone create a uniaxial hinge joint that allows just knee flexion and extension(Blackburn & Craig, 1980). A plane joint between the femur and patellar bones allows the quadriceps femoris tendon to be attached on the tibial bone and allows knee extension by minimizing maximal friction and stabilizing the knee joint.
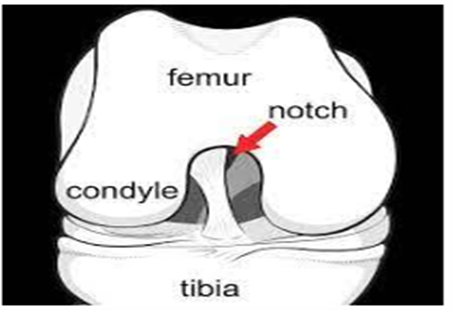
On the distal end of femur bone there is a inter condylar notch, which is extended from the posteriorly and inferiorly that separates both medial and lateral condyles of femur bone. When the condyles of femur articulate with the condyles of tibia, they are held together with two important ligaments named as
- Anterior Cruciate Ligament (ACL)
- Posterior Cruciate Ligament (PCL)
Common mechanism of injury
ACL stabilises the knee joint during high-impact activities and inhibits the forward translation and rotational movement of the tibia bone relative to the femur bone, which helps in physiological movements like running, walking, jumping, and sudden direction changes. ACL damage has a long-term influence on life, compromising quality of life and sometimes causing knee OA.

Epidemiology of injury
- Ice skiing, football players, basketball players during landing from a jump with extended knee, causes the significant increased risk of ACL injury.
- A cohort study was conducted on 1841 individuals which shows that incidence of ACL injury is 68.6 per 100000 persons per year and this incidence rate is relatively high in male than in female.